GP Connect Clinical Feature by Wayne Epton, Accredited Practising Dietician, Head of Department – Nutrition and Dietetics, Royal Perth Bentley Group
Monitoring body weight can be a quick and easy way of tracking health status and can highlight changes early. A large emphasis is placed on identifying overweight or obesity. The proportion of WA adults who are overweight or obese increases with age, from 57.4 per cent of adults aged 25 – 34 years to 76.8 per cent for older adults (>65 years)1.
However, weight management in older adults is complex, and weight reduction does not correlate with improved health outcomes in this cohort as it does in younger adults. About 25 per cent of weight loss achieved is due to a reduction in fat-free mass which can lead to sarcopenia2. Sarcopenia leads to changes in body composition, frailty and increases the risk of falls, fractures, functional dependence, and disability. Longitudinal studies show weight loss is predictive of mortality in this patient cohort.
Research indicates 40 per cent of older Australians are either malnourished or at high risk of malnutrition (undernourished). Older adults are at higher risk due to normal ageing processes that lead to altered bodily functions and is characterised as a time in the life cycle where one experiences progressive physical, cognitive, and psychosocially related functional declines.
What is a healthy weight for older adults?
In adults 18 – 65 years of age, a healthy BMI is regarded as 18.5 – 24.9kgm2 however a higher BMI in older adults provides a level of protection. Research indicates that there is a U-shaped association between all-cause mortality and BMI, with a lower risk of mortality in older adults being correlated to a BMI of 24 – 30.9kg/m23. Risk of death from any cause increases at either end of this BMI range, 37 per cent higher with a BMI less than 21kg/m2 or 18 per cent higher with a BMI greater than 35kg/m24.
An ‘obesity paradox’ has been described for the reduced mortality risk in older adults with increasing BMI. This paradox has been observed for overall mortality and disease-specific mortality, including heart failure, hypertension, coronary artery disease and stroke.
What can be done?
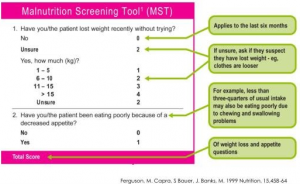 Screening nutritional status in older adults is not difficult and there are many valid and reliable nutritional screening tools available. For example, the Malnutrition Screening Tool (MST)5 has been demonstrated as reliable at identifying risk. The MST was created in Australia and is widely used in hospitals due to its ease of use. The MST consists of two questions, providing a score out of five, with a score of two or more indicating risk (see figure,left).
Screening nutritional status in older adults is not difficult and there are many valid and reliable nutritional screening tools available. For example, the Malnutrition Screening Tool (MST)5 has been demonstrated as reliable at identifying risk. The MST was created in Australia and is widely used in hospitals due to its ease of use. The MST consists of two questions, providing a score out of five, with a score of two or more indicating risk (see figure,left).
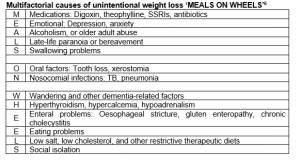
Weight loss in older adults can be multifactorial and may require some investigative work (see table, right). Social isolation and financial difficulties with the rapidly increasing cost of living are common and can be devastating when combined with other comorbidities such as diabetes, heart or kidney failure, liver or pulmonary disease, recurrent infections, or gastrointestinal disorders.
Consider referring to a dietitian for dietary education and nutrition support options for any older adults at risk. The HealthPathways WA Nutrition and Weight Management – Older Adults pathway offers advice on assessment, management and referral for patients who are:
- Overweight or obese
- Underweight
- Undernourished (regardless of weight)
- Residents of an aged care facility
References:
- Australian Bureau of Statistics (2017-18), Overweight and obesity, ABS Website, accessed 28 August 2023.
- Volpi E, Nazemi R, Fujita S. Muscle tissue changes with aging. Curr Opin Nutr Care. 2004; 7 (4): 405 – 410).
- Gill L, Bartels S, and Batsis Weight management in older adults. Curr Obes Rep. 2015 Sep; 4(3): 379–388.
- Winter J, MacInnis R, Wattanapenpaiboon N, Nowson C. BMI and all-cause mortality in older adults: a meta-analysis. Am J Clin Nutr. 2014 Apr;99(4):875-90
- Ferguson M, Capra S, Bauer J, Banks M. Development of a valid and reliable malnutrition screening tool for adult acute hospital patients. Nutrition, 1999 Jun;15(6):458-64
- Morley, JE. Cause of weight loss in Adults, Anorexia of aging: Physiologic and pathologic. American Journal of Clinical Nutrition. 1997; 66:760.