GP Connect Clinical feature by Dr Rona Kelly BMBS FRACP MPH, Paediatrician and GP Liaison Consultant, Child Development Service, and Dr Sapna Jessy MBBS (UK), FRACP General and Developmental Paediatrician, Medical Deputy Head of Department Child Development Service.
Attention Deficit Hyperactivity Disorder (ADHD) continues to be the most common neurodevelopmental diagnosis affecting children in Western Australia. Australian data shows seven per cent of children aged four to 17 years of age are affected by ADHD.1 Symptoms of ADHD can impact upon a young person’s cognitive and social development, academic achievement and daily living skills.2
Growth faltering can be defined as inadequate physical growth for age and sex, based on serial measurements.3 The risk of growth faltering is increased for children and adolescents with ADHD. This can be for many reasons, such as:
- use of S8 stimulant medicines
- executive function difficulties
- sensory sensitivities
- co-occurring neurodevelopmental or mental health conditions.
This article aims to provide GPs with an awareness of the growth faltering risk in children treated for ADHD, and to outline a stepwise approach in management and care coordination.
Growth faltering is a concern in children and adolescents with ADHD. It has an impact on brain development, immunity and energy as well as long term consequences should it persist. Medicines prescribed for the management of ADHD symptoms, particularly stimulant medicines, are associated with dose-dependent appetite suppression. This can lead to skipped meals, altered meal patterns and reduced nutritional intake. Other medication side effects include gastrointestinal disturbance and sleep issues, which can also impact a child’s willingness to eat regularly.
Stimulant medicines: Methylphenidate (short/long-acting), Dexamphetamine, Lisdexamfetamine.
Non-stimulant medicines: Atomoxetine (mild appetite effect), Guanfacine, Clonidine (weight-neutral or gain).
In addition to ADHD medicines, other factors for individuals with ADHD affecting intake include feeding behaviour difficulties, executive dysfunction (e.g. poor meal planning), sensory sensitivities (e.g. to food texture, smell or taste), increased energy expenditure and co-occurring neurodevelopmental conditions such as autism spectrum disorder (ASD) or avoidant restrictive food intake disorder (ARFID). Children at higher risk of growth faltering include those who have a starting BMI below the 5th percentile, were born preterm, have a chronic illness, have an identified eating disorder or have other environmental or family risks such as food insecurity or psychosocial complexity.4
Children and adolescents with ADHD, particularly those treated with stimulant medicines, must have regular monitoring of their growth at least every six months, including weight, height and BMI, with plotting on standardised growth charts.
Growth faltering is identified when:
- Weight or BMI measurements have crossed down one or more major percentile lines (weight loss or failure to gain expected weight).
- There is a reduced growth trend compared with previous trajectory.
- Appetite suppression is reported with inadequate compensatory intake
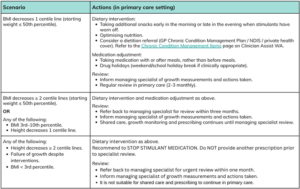
Stepwise approach for GPs in the management of growth faltering
Follow-up and relapse
Catch-up growth is common in children and adolescents after interventions such as medicine dose reduction. For all children and adolescents, it is important to maintain nutritional support and monitor closely for a rebound in weight / height trajectory. In general, BMI measurements above the 10th percentile, with normal weight gain on two evaluations, at least one month apart are reassuring for successful treatment.
Note that the risk of relapse of growth faltering is increased if the underlying aetiology is not adequately addressed. Always consider if blood tests for organic causes of poor growth are indicated at any stage, through medical and psychiatric history, family history, cultural perspectives, dietary intake, meal timing and pre-treatment appetite patterns.
In summary, children and adolescents with ADHD are at increased risk of growth faltering and require regular medical review to monitor their health and wellbeing. Appropriate recognition through growth monitoring, prompt intervention and ongoing care coordination between GPs and non-GP specialists can result in better outcomes for children, adolescents and their families.
References
- Lawrence, D., Bartlett, J., Buckingham, W., Hielscher, E., Diminic, S., & Whiteford, H. (2023). Regional estimates of child and adolescent mental disorders [Data set]. Curtin University. https://doi.org/10.25917/2JYB-PY41
- Biederman J, Monuteaux MC, Mick E, Spencer T, Wilens TE, Silva JM, et al. Young adult outcome of attention deficit hyperactivity disorder: a controlled 10-year follow-up study. Psychological Medicine. 36(2):167-79
- National Guideline Alliance (UK). Faltering Growth – recognition and management. London: National Institute for Health and Care Excellence (NICE); 2017 Sep. (NICE Guideline, No. 75.) Available from: https://www.ncbi.nlm.nih.gov/books/NBK458459/
- Hutt Vater, C., Biederman, J., DiSalvo, M., O’Connor, H., Parker, H., Woodworth, K. Y., Wozniak, J., & Faraone, S. V. (2023). Growth Trajectories in Stimulant Treated Children and Adolescents: A Qualitative Review of the Literature from Comprehensive Datasets and Registries. Journal of child and adolescent psychopharmacology, 33(9), 344–355. https://doi.org/10.1089/cap.2023.0054