By Professor Gerald F Watts and Dr Jane Purdie, from the Royal Perth Hospital Lipid Clinic, with acknowledgement to Dr. Jing Pang and Dr. Jacquie Garton-Smith.
What is the context?
Familial hypercholesterolaemia (FH) is a dominantly inherited cause of a markedly elevated level of cholesterol and is a preventable cause of premature atherosclerotic cardiovascular disease and death. Atherosclerosis caused by FH begins in childhood and needs to be detected early to prevent a coronary event.
There are approximately 100,000 people with FH in Australia, most of whom remain undiagnosed. A general practice of 10,000 patients, should on average expect to have 40 patients with FH under their care. General practice can play a major role in the detection and management of FH. There are various methods for detecting index cases with FH, including opportunistic and selective screening, in general practice. Phenotypic cases of FH will, however, require confirmation of the diagnosis genetically through referral or collaboration with a lipid clinic. Of the various detection methods for FH, the most cost-effective is cascade testing.
What is cascade testing?
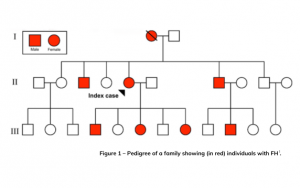
Cascade testing is a systematic way to detect blood relatives of an index case known to have FH. Because FH is an autosomal dominantly inherited condition, 50 per cent of first-degree relatives (children, siblings, parents) of an index case will have FH (see Figure 1). Cascade testing should be carried out using both genetic and cholesterol testing. An MBS item now funds pathology for GP-requested genetic cascade testing of blood relatives of an index case.
How to do genetic cascade testing?
Cascade testing is ideally carried out in a co-ordinated way, in which specialists working in lipid clinics collaborate closely with the patient’s nominated GP (see Figure 2). Genetic testing should also be carried out in the same laboratory that diagnosed the index case.
To request FH cascade genetic testing where the laboratory can bill MBS item 73353, GPs will need the genetic test result provided to them by the clinical service that has made the diagnosis in the index case. MBS items for index case testing are only available for tests referred by non-GP specialists and will typically be arranged by a lipid clinic, such as the one at Royal Perth Hospital.
A key component of cascade testing is counselling, which should involve:
- Drawing a three-generation family tree, triggered by information given by the index case’
- Obtaining informed consent for genetic testing
- Providing counselling that discusses and identifies the value of doing the genetic test
- Discussing the likely outcomes of the genetic test results and insurance implications, such as for life insurance and income protection
- Discussing the psychological sequelae of positive and negative test results
- Discussing the prognostic implications of a positive test result
All discussions should be carried out using shared decision-making.
What to do with the genetic test results?
Genetically positive patients should be referred to an adult or paediatric lipid specialist service, as appropriate. Patients will be offered enrolment into a national FH registry and triaged according to higher or lower complexity for management in tertiary and/or primary care (see Figure 2 and Figure 3).
What support is available?
The lipid clinic at Royal Perth Hospital is committed to collaborating with GPs caring for relatives of genetically defined index cases. The service aims to enable the safest and most efficient, timely and equitable way of identifying adults and children with FH, and to expedite treatment with a view to decreasing future risk of a coronary event. The two newly developed WA HealthPathways provide further information on cascade testing for FH, as well as the on assessment, management, and referral of FH.
GPs can contact the lipid clinic for clinical advice on (08) 9224 8092 or lipidclinic@health.wa.gov.au
References:
- Familial hypercholesterolaemia: A model of care for Australasia. G. F. Watts, et al. Atherosclerosis Supp 2011 Vol. 12 Pages 221-63